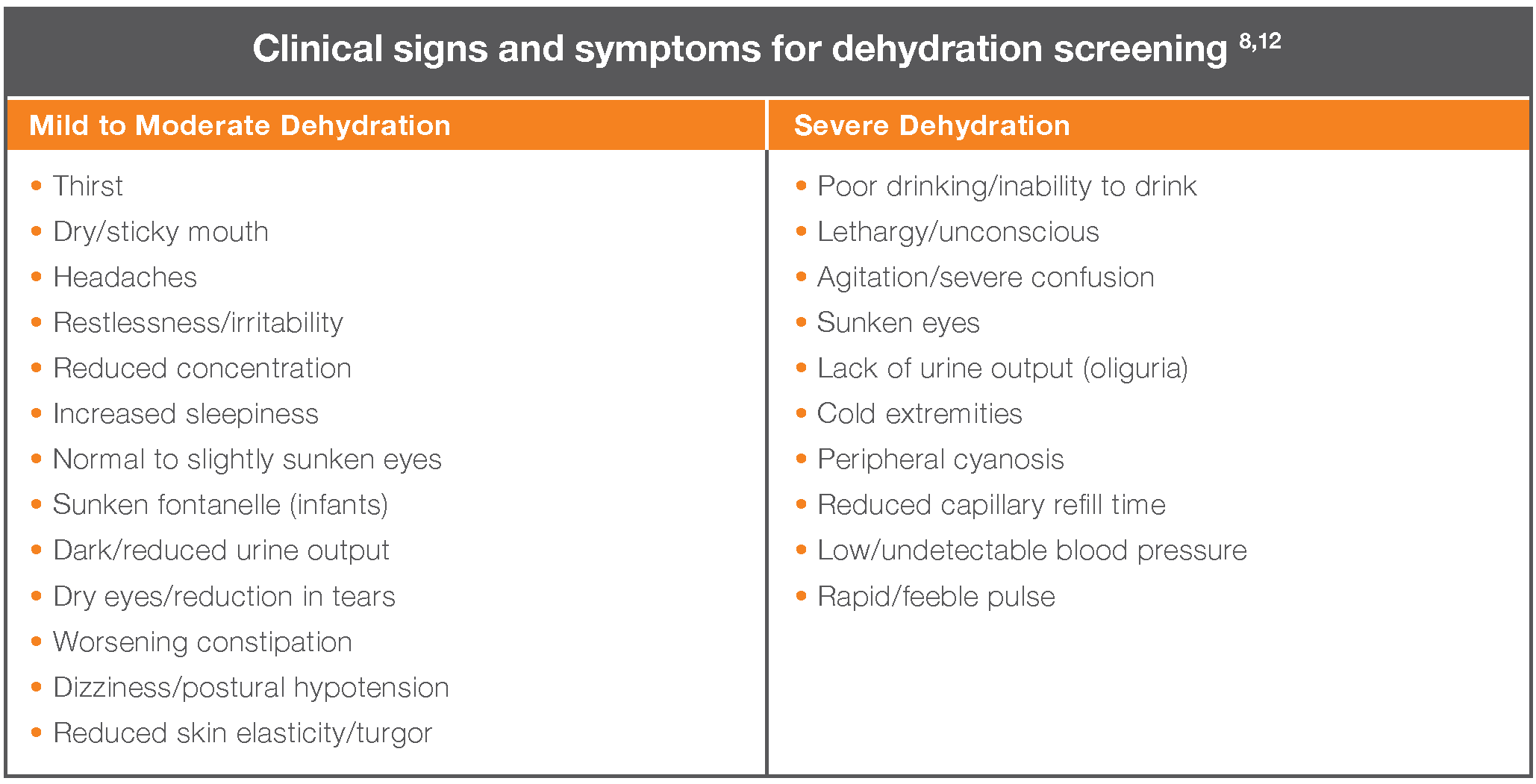
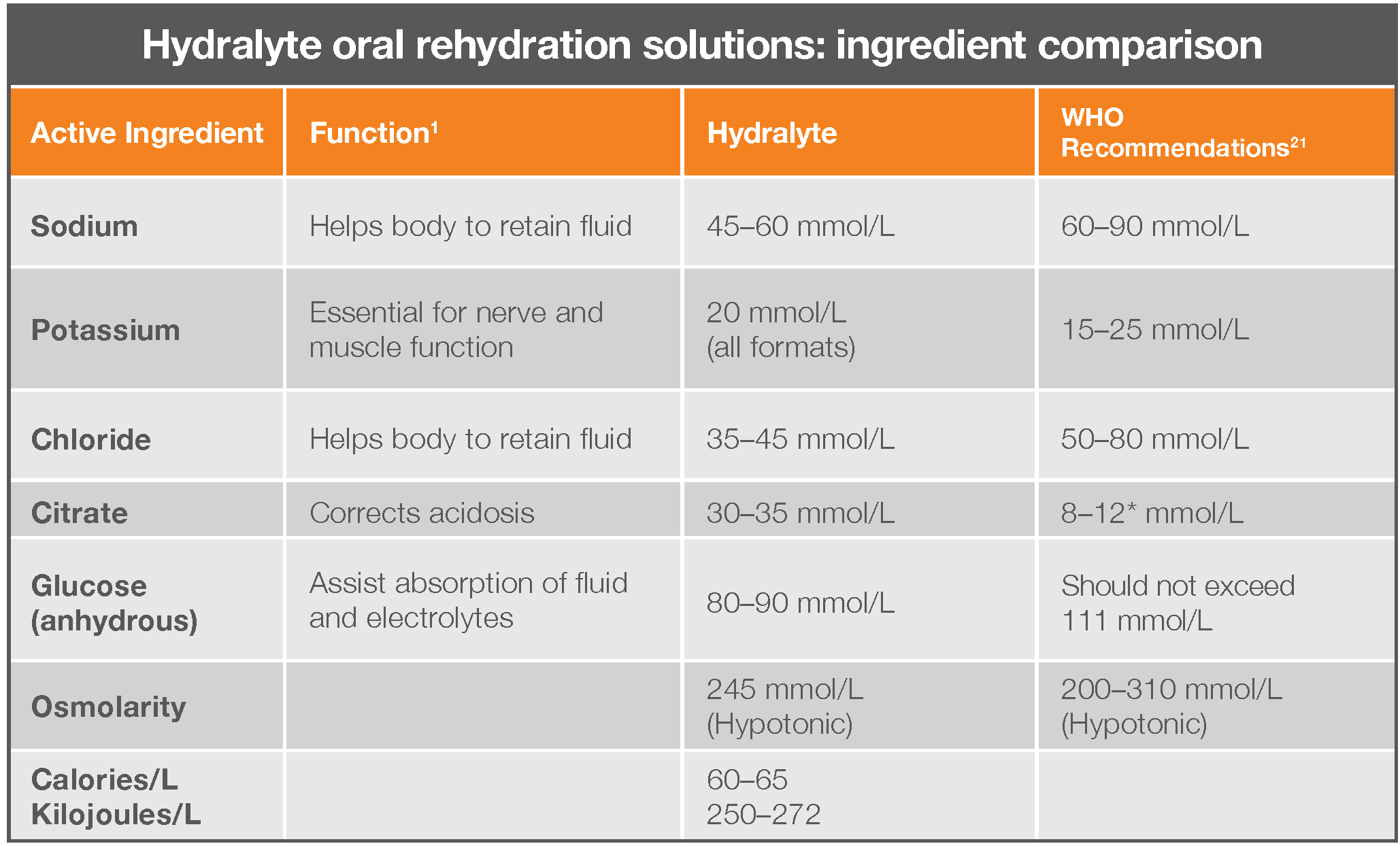
Hydralyte is specifically formulated to meet WHO ORS criteria for effective hydration.
ORS need to have an optimal balance of sodium and glucose — glucose to facilitate the absorption of sodium (and water) in the small intestine, and sodium and potassium to replace losses during dehydration.1
Using an ORS – such as Hydralyte – is a simple, proven intervention that helps rehydrate patients with mild or moderate dehydration symptoms faster than water alone.1,20
Not all ORS are the same and ORS are not the same as sports or energy drinks.
The Hydralyte range is formulated for effective hydration:
- With the correct balance of sodium and glucose in-line with WHO ORS recommendations
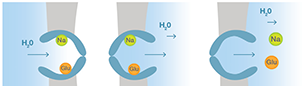 Sodium, glucose and water (by osmosis) rapidly move into the cell before being actively transported out into the bloodstream.
Sodium, glucose and water (by osmosis) rapidly move into the cell before being actively transported out into the bloodstream.
- Are hypotonic — allowing effective rehydration while minimising potential side effects such as a feeling of fullness/bloating
- Have a lower sodium content — formulated specifically for the diets of developed countries
- Contain low sugar
- Are suitable for all age populations (0–Adult)
- Available in a variety of formats and flavours