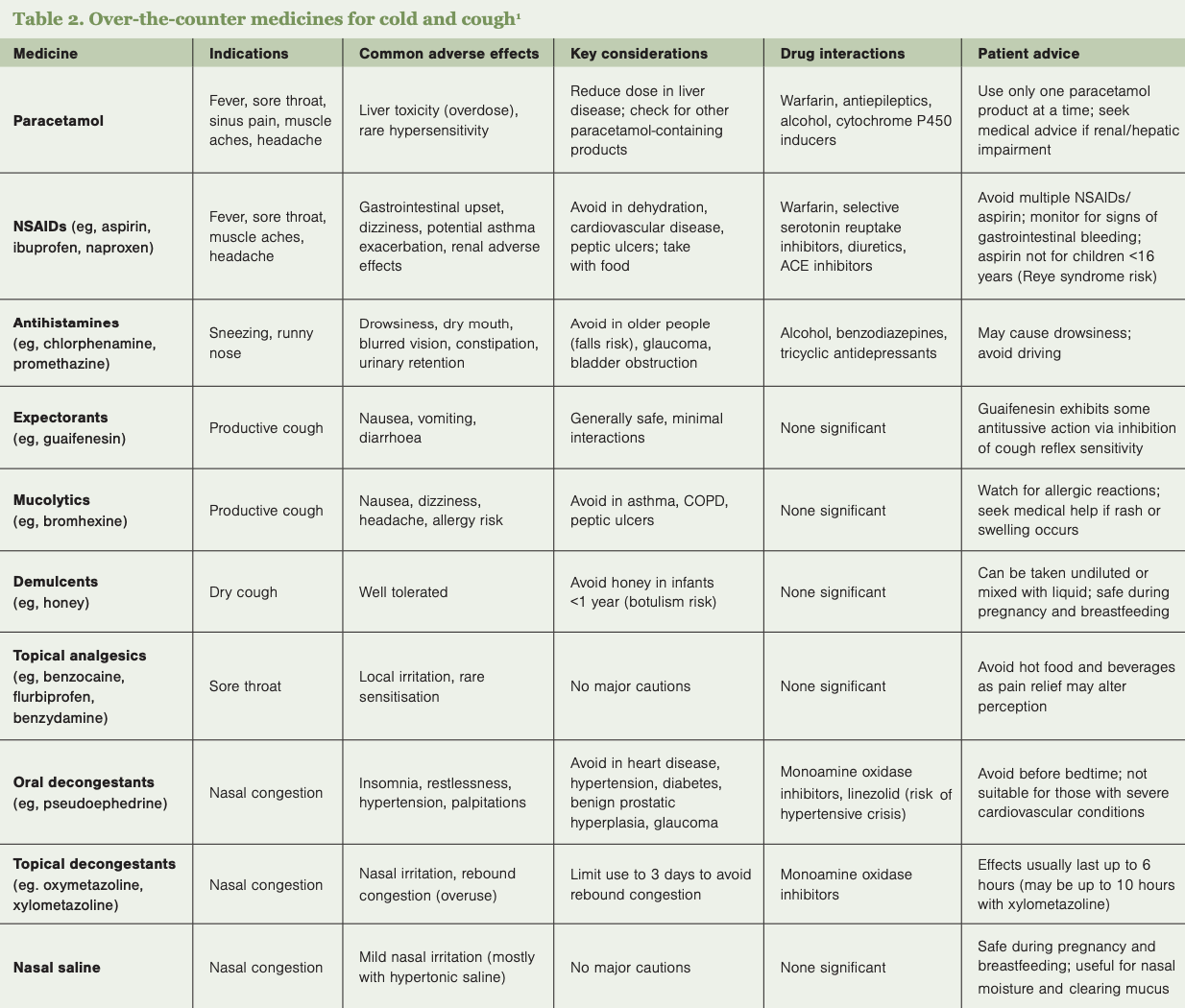
As most colds and coughs are self-limiting, a variety of over-the-counter products are used to help relieve symptoms and improve comfort until recovery (Table 2). Patients should be guided to select appropriate treatments and cautioned against the concurrent use of multiple products containing similar active ingredients to prevent overdose.
Analgesics/antipyretics – paracetamol and NSAIDs (eg, ibuprofen) are effective at managing fever, aches, headaches and sore throat. Due to its safer profile, paracetamol is the preferred first-line option for patients with multiple conditions or taking other medicines. Care should be taken to avoid exceeding the recommended dosage, especially when used with other combination cold products that contain paracetamol. Exceeding 4g of paracetamol daily can cause liver toxicity. NSAIDs carry higher risks of gastrointestinal, cardiovascular and renal side effects, especially with dehydration.4
Decongestant nasal sprays – medicines such as xylometazoline provide quick relief of nasal congestion by constricting nasal blood vessels. However, use should be limited to three consecutive days to avoid rebound congestion. More prolonged use can lead to rhinitis medicamentosa with nasal mucosa changes.1,4
Oral decongestants – pseudoephedrine is effective but may cause systemic adverse effects, such as increased heart rate and insomnia, and is contraindicated for people with severe coronary artery disease.4
Expectorants and mucolytics – these medicines aim to loosen mucus in productive coughs. Guaifenesin (expectorant) may help to expel mucus from the lungs, and bromhexine (mucolytic) may help break down thick, sticky phlegm and make it easier to cough up. However, evidence supporting either medicine’s effectiveness is limited.5
Cough suppressants (antitussives) – dextromethorphan and pholcodine were commonly used for dry, non-productive coughs. However, pholcodine-containing medicines were withdrawn in New Zealand from January 2024 due to safety concerns.6 Dextromethorphan products are no longer supplied in New Zealand, with most approvals lapsing after its reclassification in 2019 as a pharmacist-only or prescription medicine.7
Complementary treatments – aside from antitussives, which have minimal effect, no medicines effectively treat dry cough. However, complementary treatments such as honey, glycerol syrups, vapour rubs, ivy leaf extract and zinc may help reduce cough frequency or severity.2,7,8
Lozenges and throat sprays – products containing local anaesthetics, antiseptics or anti-inflammatory agents can provide temporary relief of sore throat and relieve a dry, irritating cough.